
The Two Ways to Shield Your Infant From RSV This Season
Respiratory syncytial virus (RSV) is one of the most common reasons young infants end up in the hospital during the fall and winter months. Here’s what the evidence says about how RSV prevention works, who needs it, and how to decide which option is right for your family.
There Are Two Ways to Protect Them
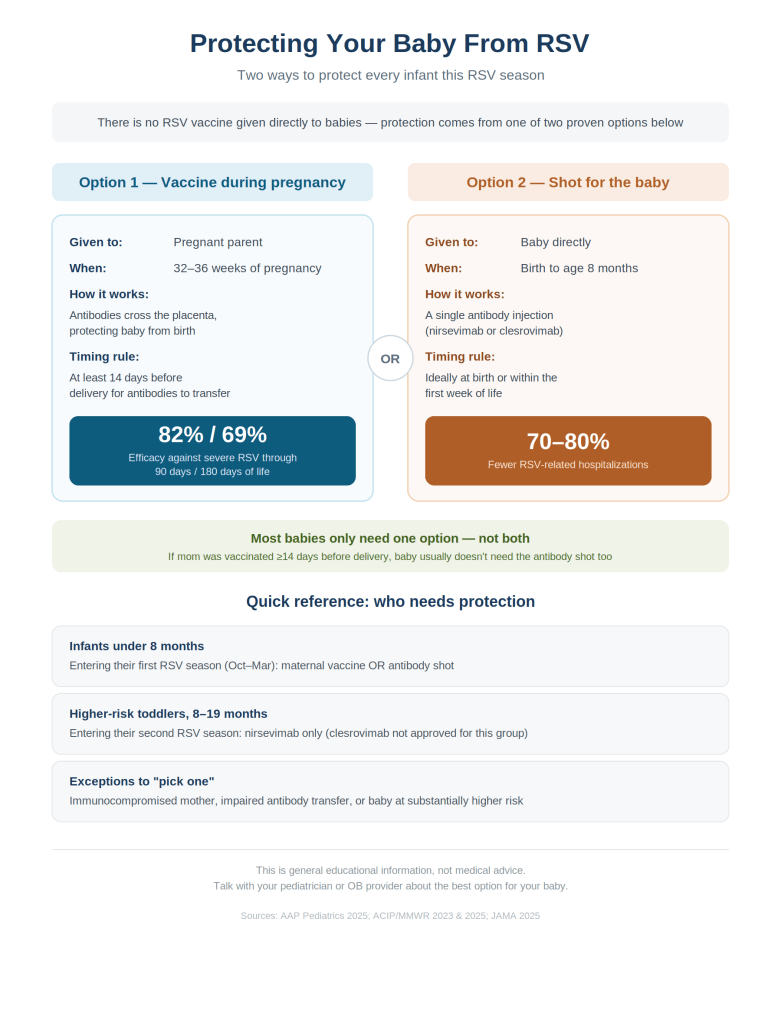
It’s a common point of confusion: there is currently no traditional RSV vaccine approved to be given directly to infants. Instead, protection comes from one of two strategies, both of which work by putting RSV antibodies into a baby’s system before they’re ever exposed to the virus.
- A vaccine given to the pregnant parent, which passes protective antibodies to the baby before birth, or
- A long-acting antibody shot given directly to the baby after birth
Every infant should be protected through one of these two routes. Neither is considered superior — the right choice depends on timing, availability, and family preference.
Option 1: RSV Vaccination During Pregnancy
The RSV vaccine for pregnant people (brand name Abrysvo) is given between 32 and 36 weeks of pregnancy, ideally at least two weeks before delivery. It works by prompting the parent’s body to produce RSV antibodies, which cross the placenta and give the baby ready-made protection from birth.
| Clinical trial results: 82% protection against severe RSV illness through the first 90 days of life 69% protection against severe RSV illness through the first 180 days of life |
Because the antibody transfer needs time to happen, this option only works if there are at least 14 days between vaccination and delivery.
Option 2: A Long-Acting Antibody Shot for the Baby
If the pregnancy vaccine wasn’t given — or wasn’t given in time — infants can instead receive a monoclonal antibody product directly. Unlike a traditional vaccine, this doesn’t train the baby’s immune system to make its own antibodies; it simply supplies ready-made antibodies that protect against RSV for several months, which is typically enough to cover a full RSV season.
Two products are currently available:
- Nirsevimab (Beyfortus) — approved for infants entering their first RSV season, and for certain higher-risk toddlers (8–19 months) entering their second season
- Clesrovimab (Enflonsia) — approved for infants entering their first RSV season only
Both are given as a single intramuscular injection, ideally during the birth hospitalization or within the first week of life for babies born during RSV season. They can be given at the same visit as routine childhood vaccines, so there’s no need for a separate appointment.
| Real-world data show these antibody shots reduce the risk of RSV-related hospitalization by roughly 70–80%. |
Who Needs Which — and When
- Infants under 8 months, born during or entering their first RSV season (typically October through March): should receive either maternal vaccination (if timed appropriately) or an antibody shot.
- Children 8–19 months at increased risk for severe RSV, entering their second RSV season: nirsevimab is recommended (clesrovimab is not approved for this group).
- Most families only need one or the other, not both. If the pregnant parent received the RSV vaccine at least 14 days before delivery, the baby generally does not need an additional antibody shot.
When a Baby Might Need the Antibody Shot Even After Maternal Vaccination
There are a handful of situations where a doctor may still recommend the infant antibody shot even if the pregnancy vaccine was given:
- The mother is immunocompromised
- A medical condition affected how well antibodies transferred to the baby
- The infant is at substantially increased risk for severe RSV disease
If any of these apply, it’s worth a direct conversation with your doctor about whether additional protection makes sense.
Which Option Should You Choose?
No single product is considered preferred over the others. The right choice comes down to practical factors: when in pregnancy you’re able to get vaccinated, when your baby is due relative to RSV season, what’s available at your clinic or hospital, and your own preference as a parent. Either path — done on time — gives your baby strong protection through the riskiest months of early life.
The Bottom Line
RSV can be serious in young infants, but prevention has come a long way. Whether protection comes from a vaccine during pregnancy or an antibody shot after birth, the key is making sure your baby is covered by one of these options before RSV season arrives. Talk to your OB or pediatrician early — ideally before the third trimester — about which route fits your timeline.
Related: Medical Myths or Facts #26: Does RSV Vaccination During Pregnancy Improve Infant Outcomes?, For Parents
References
- Committee on Infectious Diseases. Recommendations for the Prevention of RSV Disease in Infants and Children: Policy Statement. Pediatrics. 2025.
- Jones JM, et al. Use of Nirsevimab for the Prevention of RSV Disease Among Infants and Young Children: ACIP Recommendations. MMWR. 2023.
- Moulia DL, et al. Use of Clesrovimab for Prevention of Severe RSV-Associated LRTI in Infants: ACIP Recommendations. MMWR. 2025.
- Jabagi MJ, et al. Nirsevimab vs RSVpreF Vaccine for RSV-Related Hospitalization in Newborns. JAMA. 2025.
- Fleming-Dutra KE, et al. Use of the Pfizer RSV Vaccine During Pregnancy for the Prevention of RSV-Associated LRTD in Infants: ACIP Recommendations. MMWR. 2023.





Leave a comment